
Patellofemoral Pain in London: Causes, Diagnosis and Evidence-Based Treatment (2026 Definitive Guide)
Introduction

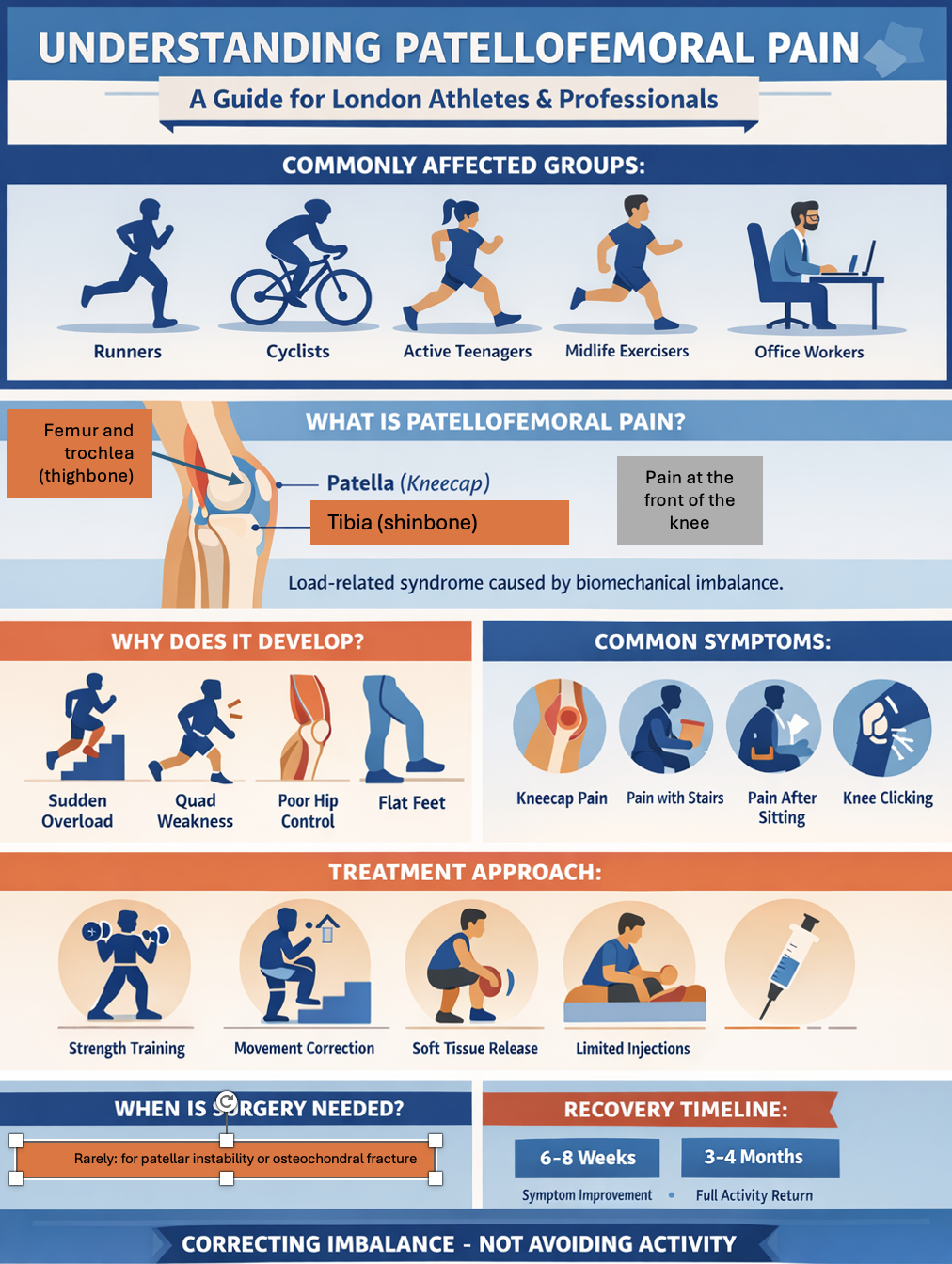
Patellofemoral pain, often called runner’s knee, is a common cause of anterior knee pain caused by irritation between the kneecap (patella) and the femur. It usually develops due to muscle imbalance, overtraining, or poor movement mechanics rather than structural damage.
Patellofemoral pain is one of the most common causes of anterior knee pain in:
Runners
Cyclists
Teenagers in sport
Midlife active adults
Office-based professionals with load imbalance
It is often labelled loosely as:
“Runner’s knee”
“Chondromalacia”
“Anterior knee pain”
However, patellofemoral pain is not a single diagnosis. It is a load-related syndrome driven by biomechanical imbalance.
In London, where participation in recreational sport, commuting load, and gym training are high, patellofemoral pain is frequently seen in both athletes and professionals.
This guide explains:
What patellofemoral pain actually is
Why it develops
When imaging is required
How it differs from cartilage damage
Evidence-based treatment
When surgical intervention is appropriate
The objective is to correct muscle and biomechanical imbalances rather than aim for injections and antiinflammatory suppression.
What Is Patellofemoral Pain?
The patellofemoral joint is formed between:
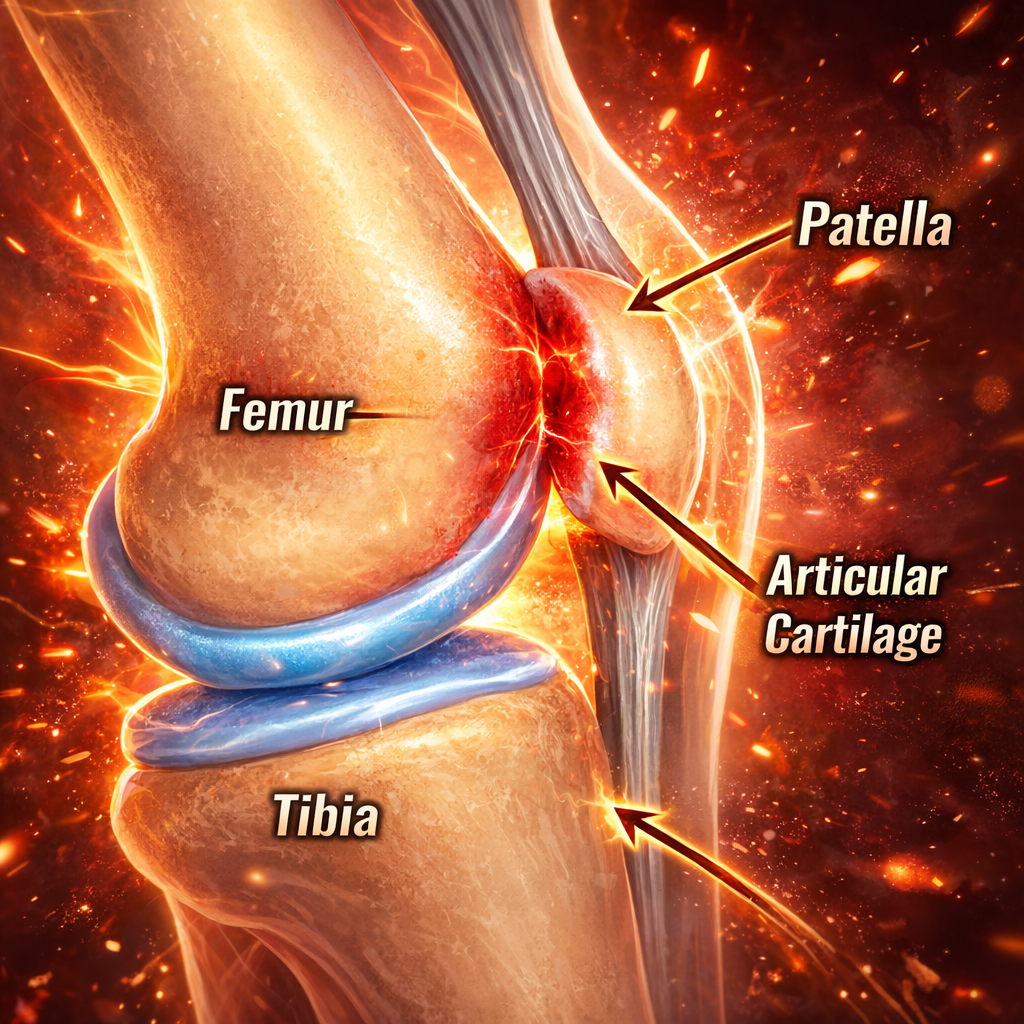
The patella (kneecap)
The trochlear groove of the femur (thigh bone)
If the femur (thighbone) is 2 wheels on the tibia (a bumpy road), then the patella is like a brake pad at the front.
Pain arises when:
Load exceeds tissue tolerance: this can be from overtraining, increasing intensity of training too quickly, or simply bad posture when sitting on standing for long periods of time.
Patellar tracking is suboptimal
Muscle imbalance alters force distribution
It is typically a functional overload or repetitive stress syndrome, not a structural injury..
Common Symptoms
Pain around or behind the kneecap
Discomfort with stairs
knee pain after sitting long time
Pain with squatting or lunging
Occasional crepitus
Swelling is usually minimal.
True locking (inability to straighten the knee) is absent.
Instability (the knee feeling wobbly or giving way) is uncommon unless patellar dislocation is present.
Why Does Patellofemoral Pain Develop?
1. Load Mismatch
Sudden increase in:
Running volume
Hill training
High-intensity classes
Deep squatting lunging or high impact jumping or landing, with poor form or when fatigued
The patellofemoral joint experiences high compressive force in deep flexion.
2. Quadriceps Imbalance
Weakness or delayed activation alters patellar mechanics.
The vastus medialis obliquus may not sufficiently stabilise the patella.
3. Hip and Pelvic Control
Poor hip abductor (“glute”) strength increases dynamic valgus.
Dynamic valgus increases lateral patellar load.
4. Biomechanical Alignment
Excessive femoral internal rotation or flat footed (pronation) patterns can increase patellofemoral stress.
5. Deconditioning in Midlife
In white collar professionals who sit for lon periods and then return to high-intensity exercise after years of lower load exposure, the patellofemoral joint may be underprepared.
What else can cause anterior knee pain?
fat pad impingement
ilitiobitibial and syndrome
referred pain from the back lumber spine L3/L4
referrred pain from the hip
When Is Imaging Required?
X-rays will only show bones and large bone issues such a fractures
MRI is indicated if:
Swelling persists
True instability (giving way) or catching sensation occurs
Symptoms fail to improve after a structured biomechanical rehabilitation and physio program
There is suspicion of cartilage defect or osteochondral lesion in the patella or femur
In many cases, imaging is normal or shows minor cartilage signal change.
Clinical assessment with an anterior knee pain specialist London remains the kay way of assessing and diagnosing the issue.
Differentiating Patellofemoral Pain from Structural Cartilage Damage
Patellofemoral pain syndrome:
Load-dependent: usually worse when loading in flexion eg squats, lungs or kneeling or going up and downstairs
Minimal swelling
Reversible with rehabilitation
Structural patellofemoral cartilage defect:
Persistent knee swelling or effusion
Mechanical symptoms of sharp pain, catching locking or giving way.
If there Is a clear suspicion of this or pain is not improving, it is important to get a clinical assessment from a sports doctor or knee surgeon and imaging with MRI and possibly Xray
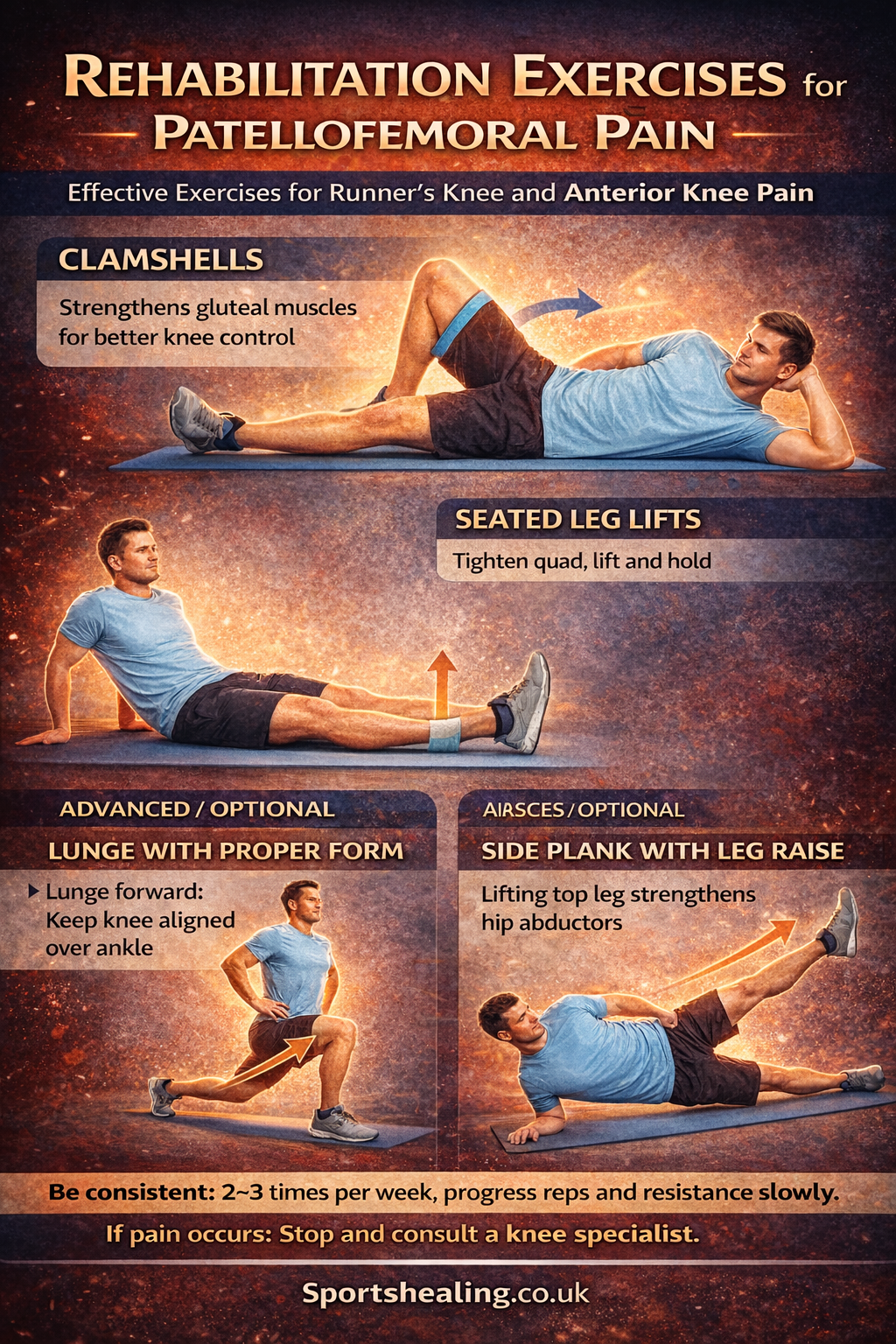
Evidence-Based Treatment
Best exercises for patellofemoral pain
1. Load Modification
Temporary reduction in:
Deep flexion exercises
Downhill running
Stair repetition
Not permanent avoidance. Structured reloading is essential.
2. Progressive Strength Training
Focus areas:
Quadriceps
Hip abductors
Gluteal complex
Core stability
Isolated VMO exercises alone are insufficient.
Integrated kinetic chain strengthening is required.
3. Movement Retraining
Correct:
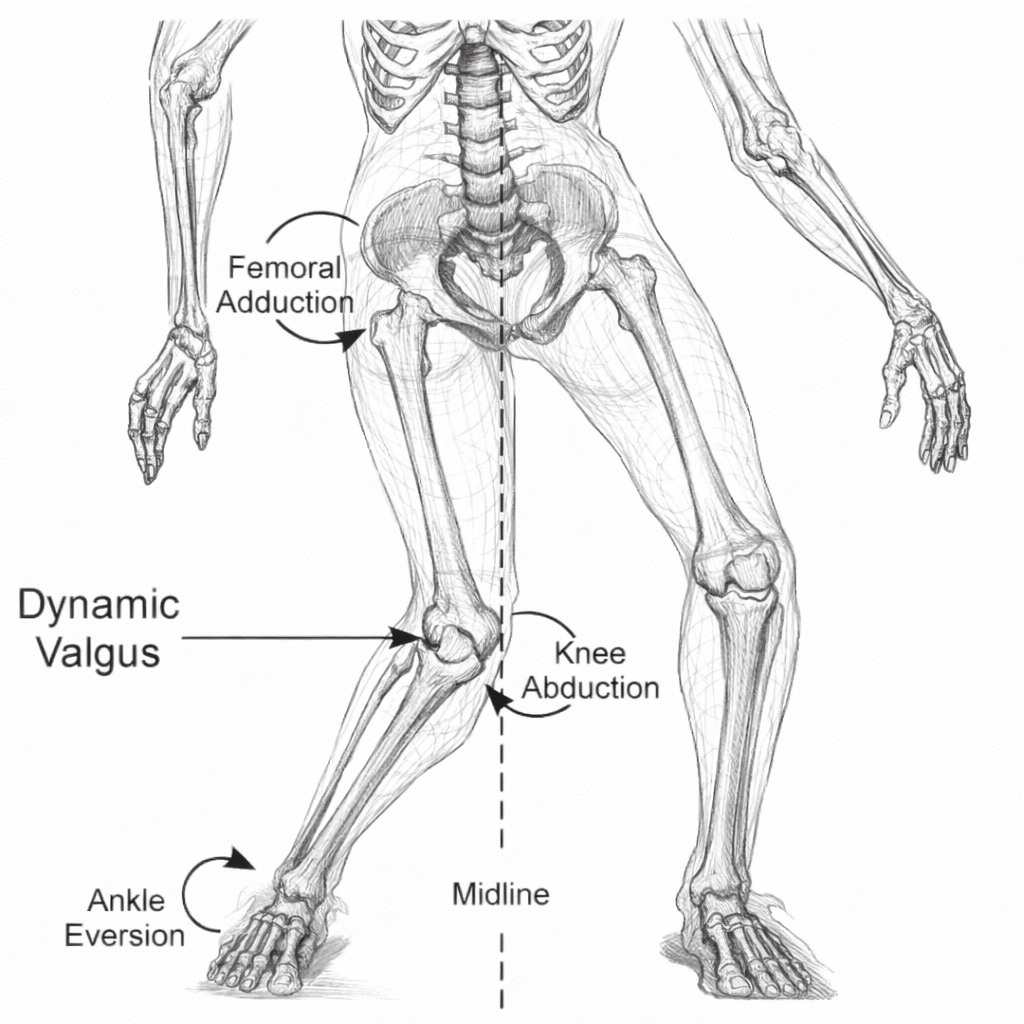
Dynamic valgus collapse
Excessive hip internal rotation
Poor squat mechanics
Technique correction reduces patellofemoral stress.
4. Soft tissue release and patellar taping
Releasing the pressure around the kneecap can be done with a good stretching and fascial release program. This can include:
hamstring stretches
iliotibial band stretches and releases
Quadriceps and calf muscle stretches
acupuncture and massage can help this
Short-term taping may reduce pain and improve neuromuscular engagement.
Bracing usually does not help in the long term
5. Injection Therapy
In selected cases with inflammation of the fat pad, or iliotibial band:
Ultrasound targeted corticosteroid may provide short-term relief
Hyaluronic acid or PRP evidence remains variable
Injections should not replace rehabilitation.
When Is Surgery Considered?
Rarely indicated in isolated patellofemoral pain without structural abnormality.
Surgical options may be considered in:
Recurrent patellar instability
Significant trochlear dysplasia, patella alta (high riding patella)
Large cartilage defects
Malalignment requiring realignment
Very tight ITB resistant to all other conservative measures; this can be released lengthened
Surgery is for if there is structural correction required,, not simply for pain suppression.
Patellofemoral Pain in Adolescents
Common in:
Teenage girls
Rapid growth phases
High training load
Early neuromuscular training prevents chronicity.
Patellofemoral Pain in London Runners
Common triggers:
Sudden mileage increase
Hill repetition
Hard pavement running
Poor recovery scheduling
poor footwear for individual biomechanics
Structured periodisation reduces recurrence.
Recovery Timeline
The good news is that most PF pain can be improved and managed with physio and biomachnical corrections and With structured rehabilitation:
Symptom improvement: 6–8 weeks
Full load return: 3–4 months
The bad news is that recurrence is common if strengthening is discontinued.
Prevention Strategy
1. Gradual load progression
2. Strength training twice weekly
3. Avoid abrupt training spikes
4. Maintain hip strength
Patellofemoral pain reflects load error, not joint failure.
Frequently Asked Questions
What is patellofemoral pain?
Patellofemoral pain is pain arising from the joint between the kneecap and the femur, usually caused by load imbalance or muscle weakness rather than structural damage.
Why does my knee hurt when I go up stairs?
Pain on stairs is common in patellofemoral pain because the kneecap experiences higher compressive forces when the knee bends deeply.
Does kneecap pain mean arthritis?
No. Patellofemoral pain is usually a biomechanical overload problem rather than degenerative arthritis.
How long does patellofemoral pain take to recover?
Most patients improve within 6–8 weeks with physiotherapy and strengthening, although full return to activity may take 3–4 months.
Do I need an MRI for patellofemoral pain?
MRI is usually only required if symptoms persist, swelling occurs, or cartilage injury is suspected.Is patellofemoral pain arthritis?
No, not usually. It is typically a load-related repetitive stress and pain syndrome rather than degenerative joint collapse.
Does knee clicking and cracking mean cartilage damage?
Usually not: Crepitus without swelling or locking is common and not necessarily pathological.
Should I stop running if I have patellofemoral pain?
That depends on severity on pain, and the terrain that you are running on. Red flags include: Persistent knee swelling or effusion
Mechanical symptoms of sharp pain, catching locking or giving way.
If there Is a clear suspicion of this or pain is not improving, it is important to get a clinical assessment from a sports doctor or knee surgeon and imaging with MRI knee scan and possibly Xray
Temporary modification may help, but complete cessation often worsens deconditioning.
Conclusion
Patellofemoral pain is not uncommon in active people who run, jump, cycle and land in flexion..
It reflects load imbalance and neuromuscular control deficits.
Most cases respond to structured rehabilitation.
Surgery is rarely required.
Correction of mechanics, not avoidance of movement, restores function.