
Children’s ACL Injury in the UK: Diagnosis, Growth Considerations and Treatment Strategy (2026 Definitive Guide)
Introduction
Anterior cruciate ligament (ACL) injuries in children and adolescents have increased substantially across the UK and in the world over the past decade.
Contributing factors include:
Early sport specialisation
Year-round competition
Increased intensity in academy-level sport with less rest periods
Greater participation of girls in pivoting sports often with poorer facilities
Better access to MRI enabling earlier diagnosis when suspected
Unlike adult ACL injuries, paediatric ACL tears must be managed with consideration of:
Open growth plates
Long-term bone joint development
Secondary meniscal injury risk
Psychological impact of stopping playing sport in children, whose whole identity as school may be affected by this.
This guide explains:
How ACL injuries present in children
How diagnosis differs from adults
Growth plate considerations
Surgical versus non-surgical management
NHS versus private pathways in the UK
Long-term joint protection
The objective is precision management that protects both growth and cartilage and restores children to playing the sports they love to play.
Why are Children’s ACL Injuries increasing?
Several epidemiological trends are clear:
IIncreased exposure to high-risk cutting sports
Higher training frequency and intensity
Improved diagnostic awareness with availability of MRI knee scans
Greater participation of young females in pivoting sports, often with poorer training regimes and facilities
Girls aged 13–17 show particularly elevated risk. Although exact causes remain unclear, this may be due to:
Neuromuscular control patterns
Hormonal influences
Biomechanical valgus tendencies
Poorer pitch and training facilities and the “gendered environment”
This is now a recognised UK public health concern in youth sport.
What are the signs of ACL injury in children and teenagers?
Typical features:
Twisting injury with foot planted not the ground or with ski not releasing
Audible “pop”
Immediate swelling within hours
Instability or giving way
Reduced confidence in pivoting
Children may under-report instability.
Recurrent swelling after sport is a key indicator.
How do you diagnose a child’s ACL injury?
Clinical Examination
Includes:
Lachmann and anterior drawer test child
Lachman test
Pivot shift
Effusion assessment
Examination can be difficult in anxious adolescents.
MRI Imaging
MRI confirms:
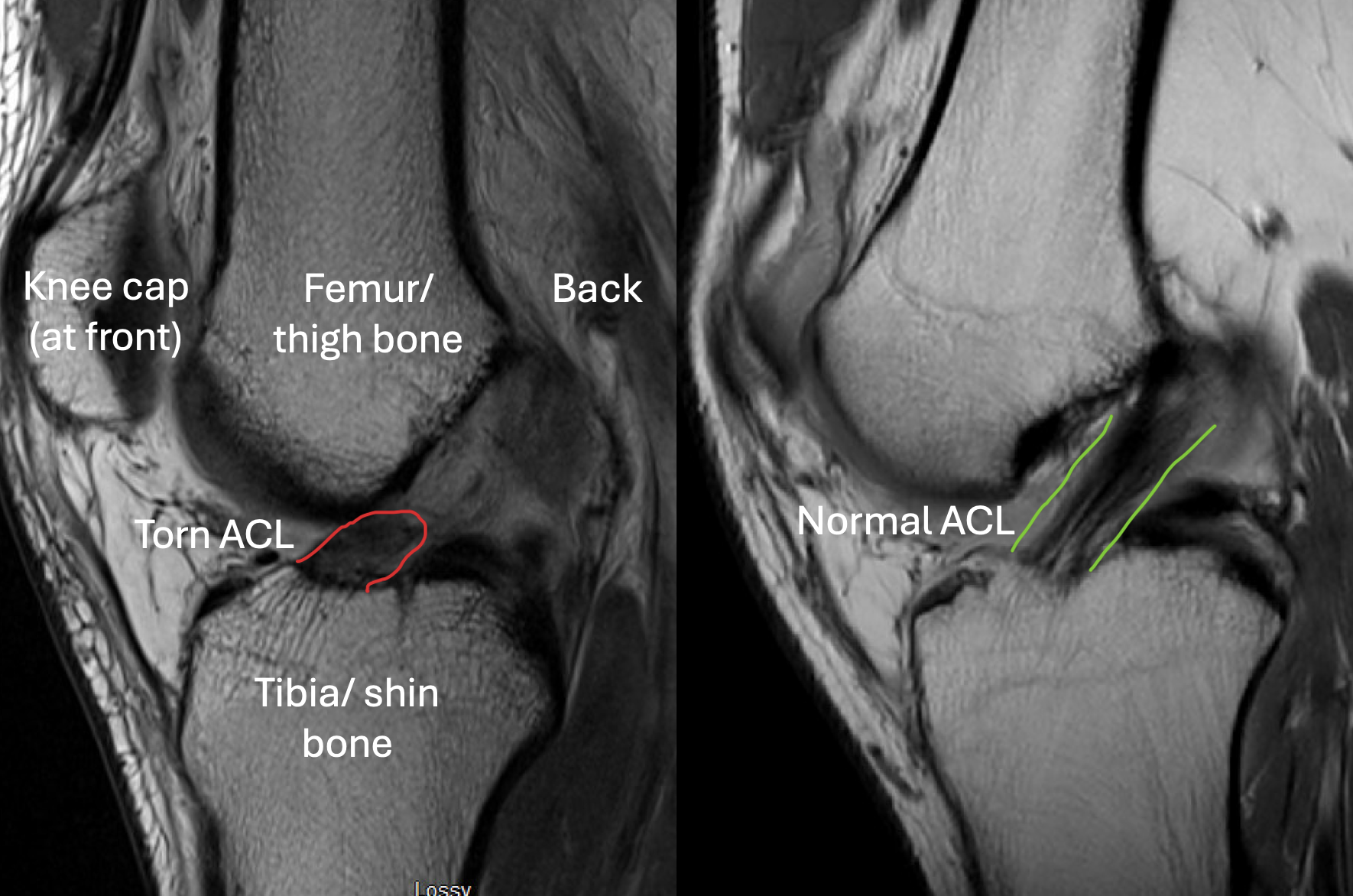
ACL rupture
Meniscal tears
Cartilage injury
Bone bruising
High-quality imaging is essential. To book an MRI click here
Delayed imaging risks missing meniscal tears.
Growth Plate Considerations
Children have open physes (growth plates) around the knee at:
Distal femur
Proximal tibia
Traditional adult ACL reconstruction techniques risk physeal injury if not modified.
Excessive damage to the growth plates may cause:
Growth disturbance
Limb length discrepancy
Angular deformity
Specialised paediatric ACL techniques are required.
Non-Surgical Management of children and teenagers’ ACL injuries
Historically, some children were treated with bracing and physiotherapy alone.
However, evidence shows:
High rates of recurrent instability after return to sport
Higher rates of meniscal injuries in non surgically treated children who return to sport
Secondary meniscal tears
Accelerated cartilage damage
Non-operative management may be appropriate in:
Low-demand children
Partial tears
Skeletally near-mature adolescents
But unstable pivoting athletes often require reconstruction.
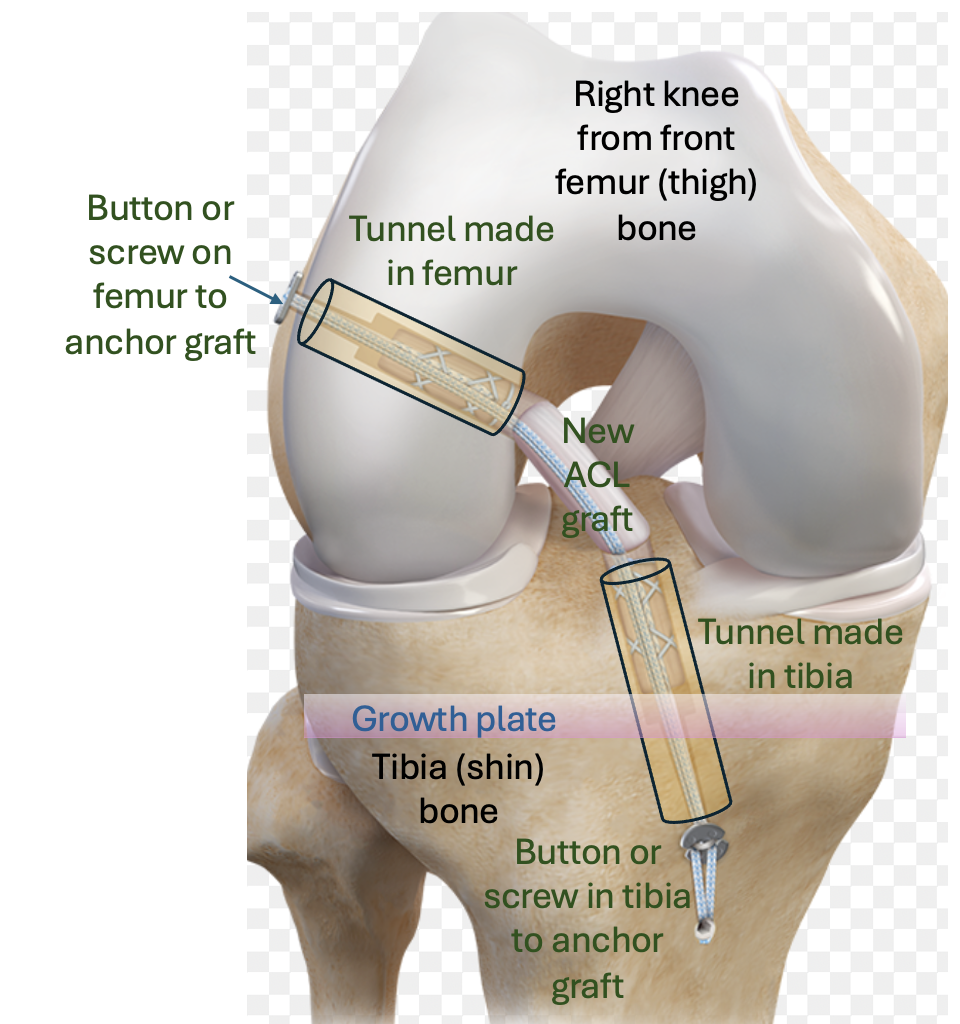
Surgical Options in Children
1. Physeal-Sparing Techniques
Avoid drilling across growth plates.
Used in younger children with significant growth remaining.
2. Transphyseal Reconstruction
Carefully placed tunnels across physes.
Safe when performed with precision and appropriate technique.
Often used in adolescents approaching skeletal maturity.
Read more about this here
Graft Choice in Paediatric ACL Surgery
Common options:
Hamstring autograft
Quadriceps tendon autograft
Patellar tendon teenagers who are skeletally mature
Live donor from parent
Graft selection must account for:
Growth
Sport
Revision risk
Long-term stability
Allograft is generally avoided in young high-demand patients due to higher failure risk.
Risks of Delayed Surgery
Delayed stabilisation may increase:
Medial meniscal tears
Meniscal root injury
Cartilage damage
Early osteoarthritis risk
Each episode of instability can cause secondary damage.
Timely assessment protects the joint.
NHS vs Private Pathways for children’s ACL injuries in the UK
NHS
* Free at point of care
* Regional paediatric specialist centres
* Waiting times vary
Private
Faster access
Direct consultant continuity
Typical cost range: £10, ,000–£18,000
Paediatric expertise matters more than setting.
Rehabilitation After Surgery
Rehabilitation is structured and gradual:
Protected early phase
Progressive strengthening
Neuromuscular retraining
Objective return-to-sport testing
Return to pivoting sport typically:
9–12 months minimum.
Too Early a return increases re-rupture risk.
Risk of Re-Injury in Young Athletes
Adolescents have higher rates of:
Graft re-rupture
Contralateral ACL injury ie injury to the other knee (10-20%)
For an example of a typical children’s ACL rehab program click here
Prevention programmes must continue after surgery.
Time alone does not confer readiness.
Objective strength symmetry and movement quality are essential.
Psychological Considerations
ACL injury in teenagers can lead to:
Anxiety about return
Loss of athletic identity
Reduced confidence
Integrated psychological support improves outcomes.
Long-Term Implications
ACL injury before adulthood increases risk of:
Meniscal deficiency
Cartilage thinning
Early osteoarthritis
Joint preservation strategy must begin at first injury.
Decision Framework for Parents
Ask:
1. Is the knee unstable?
2. Is the child involved in pivoting sport?
3. Are growth plates open?
4. Is there meniscal damage?
5. What surgical technique protects growth?
6. Is it a partial or complete ACL injury?
7. What are the risks of surgical and non surgical management.
Early specialist paediatric evaluation is essential.
Here is an expert consensus statement
Frequently Asked Questions
Is ACL surgery safe in children?
Yes, when performed using growth-aware techniques by experienced paediatric knee surgeons.
Can children return to competitive sport?
Many do, but structured rehabilitation and objective return criteria are critical.
What happens if surgery is delayed?
Repeated instability episodes may increase meniscal and cartilage damage.
Conclusion
Children’s ACL injuries require specialised assessment.
Management must balance:
Growth plate protection
Joint stability
Cartilage preservation
Safe return to sport
Early precision reduces long-term risk.